

What Is The False Claims Act And How Does It Impact Providers Of Health Care Services?
The Touch of the Affordable Care Act on the Health Care Workforce
The Impact of the Affordable Care Human activity on the Health Care Workforce
March 18, 2014 29 min read Download Report
Summary
An estimated 30 million Americans are expected to gain health insurance through the Affordable Care Deed (ACA), and a salubrious and sizable workforce will be needed to meet the increased demand. The health intendance workforce is already facing a critical shortfall of health professionals over the side by side decade. The ACA breaks the promises of access and quality of care for all Americans by escalating the shortage and increasing the burden and stress on the already delicate system. The ACA's attempts to address the shortage are unproven and limited in scope, and the significant financial investment will not produce results for years due to the training pipeline. With the ACA'due south estimated 190 million hours of paperwork annually imposed on businesses and the wellness care industry, combined with shortages of workers, patients volition exist facing increasing expect times, limited access to providers, shortened time with caregivers, and decreased satisfaction. The health care workforce is facing increased stress and instability, and a major redesign of the workforce is needed to extend care to millions of Americans.
Central Takeaways
The Affordable Intendance Human action (ACA) exacerbates the growing health care workforce shortage.
Health care workers are facing mounting stress and instability as the Affordable Care Act forces industry changes that overburden health professionals.
The ACA will impose 190 million additional hours of paperwork annually, limit fourth dimension with patients, and insert government into the patient–provider relationship.
I worry well-nigh giving 30 million people a card and a simulated promise.[1]
—Dr. Atul Grover, Principal Public Policy Officer American Association of Medical Colleges
The Affordable Intendance Act of 2010 (ACA) is projected to aggrandize health insurance coverage to an estimated xxx million to 34 million people. However, expansion of coverage is not an expansion of actual care, and the distinction is becoming clear.[2] When Congress enacted the national wellness constabulary, information technology unleashed a potential tsunami of newly insured patients, flooding a delivery system that was already strained and fragile. The American health care infrastructure has had workforce shortages for decades and is non prepared to see such a vast influx of patients effectively or efficiently. Training new physicians, nurses, and other health professionals takes years, sometimes decades. Without more graduates from nursing and medical schools and increased innovation in shared roles and responsibilities amid doctors, nurses, and other medical professionals, individuals and families will confront longer wait times, greater difficulty accessing providers, shortened fourth dimension with providers, increased costs, and new frustrations with intendance commitment.
A system overload is inevitable. Pent-up demand from those waiting for a plastic card and attracted by the promise of "free" or heavily subsidized services is expected. Of course, doctors, nurses, and other medical professionals want to help people in need, merely the sheer logistics of expanded intendance delivery, the current and growing shortage of personnel, and limited resources volition certainly undercut the good intentions of the policymakers who crafted the national health law. In fact, the "transformational" changes touted by the law'due south champions will likely complicate and negatively touch wellness care workers and their power to provide care. These changes will increase regulatory burdens, increment already heavy workloads, reduce payments, impose new penalties, and disregard personal preferences and values. The increased stress will further destabilize the health care industry. These factors combined will threaten access and quality of treat all Americans, thus breaking the President'due south promises and the stated intentions of those in Congress who enacted the national health law.
Making a Bad Situation Worse
Despite the best efforts of medical professionals and educators to increase the workforce over the past few years, shortages are projected in every health care profession. The projected supply of workers fails to meet the demand associated with population growth and aging of the population. With the new demand for medical services for the millions who are expected to enroll in Medicaid and the federal and state insurance exchanges, the workforce shortages could become catastrophic.
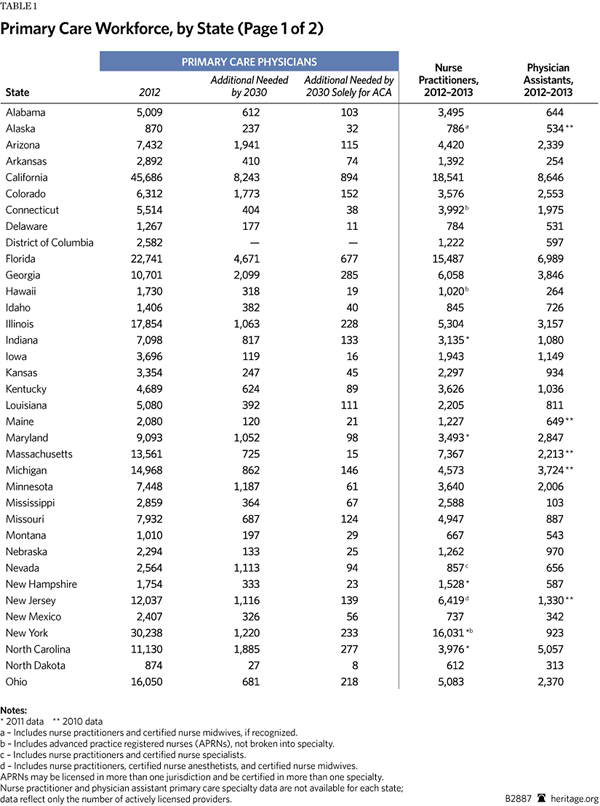
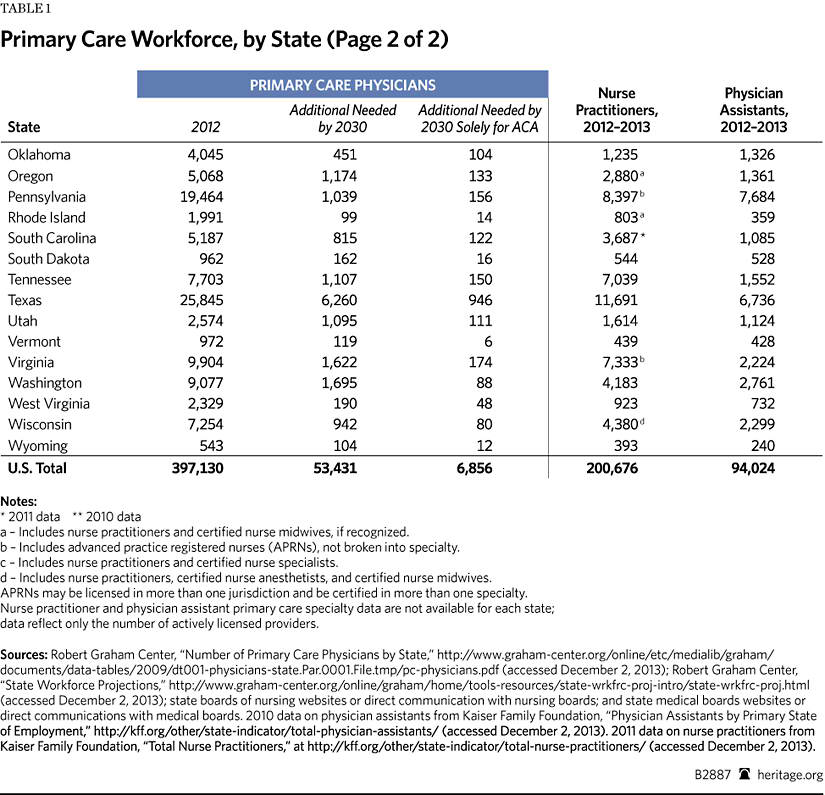
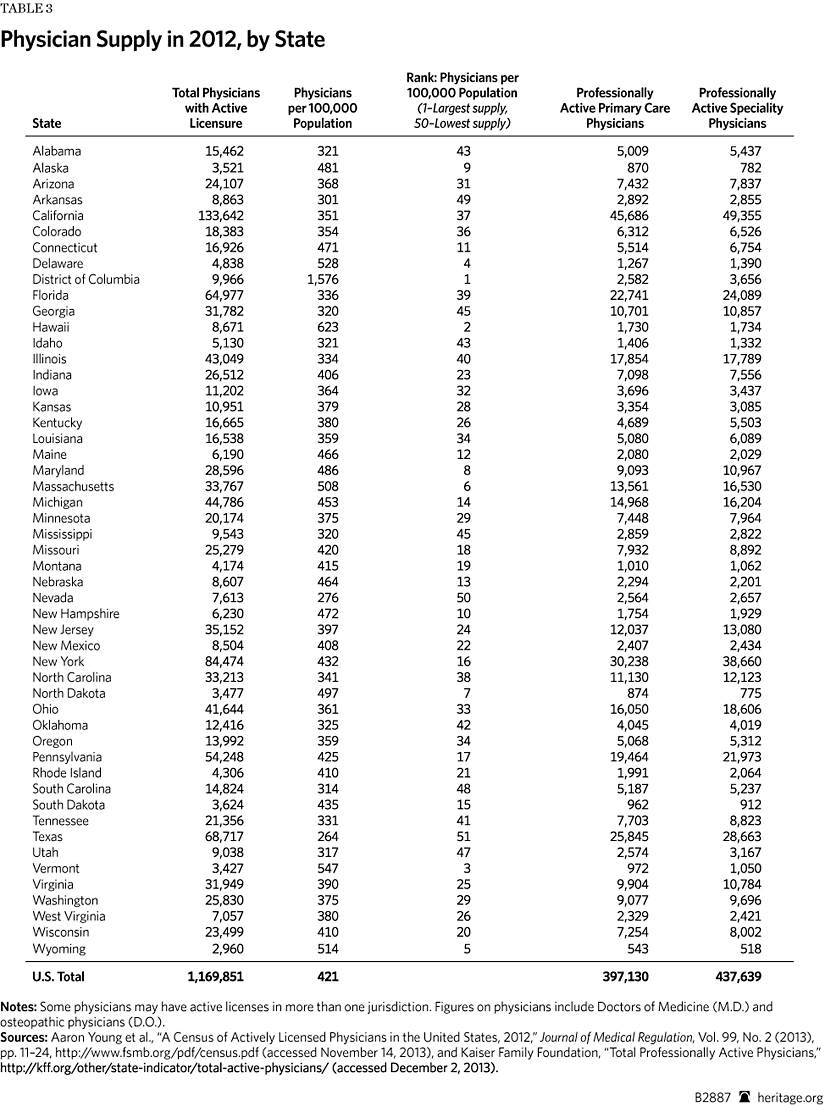
Based on a 2012 compilation of country workforce studies and reports, every state clearly needs more physicians. In that location are shortages of primary care physicians and specialists.[3] All health professions are facing personnel shortages: dental, mental wellness, pharmacy, and allied health—to proper name a few. Before the ACA's enactment, a confluence of pressures had contributed to labor forcefulness problems. The ACA will impose additional strains on the health intendance workforce.
Population Demographics. The current U.Due south. population is more than 315 1000000 and growing.[4] By 2030, 72 million Americans will be 65 or older, a l percent shift in age demographics since 2000.[five] The shift is mostly due to the crumbling baby boomers, who were born at the conclusion of World State of war Two. Americans are living longer than ever before with the help of breakthroughs in medical technology and advanced care management. Seniors currently account for 12 percent of the population but will account for 21 percent by 2050. This growing, aging population will ensure more than chronic illness and additional stress on the health care workforce.[half dozen]
Distribution Shortfall. A maldistribution trouble already exists. In much of the nation, wellness professionals are highly concentrated in urban locations.[7] The federal authorities established Wellness Professional Shortage Areas (HPSAs) in 1976, pursuant to congressional enactment of the Wellness Professions Educational Assistance Act, to increase the number of wellness care workers in rural and underserved areas. Nevertheless, 37 years afterwards, admission to care is still unequal between urban and rural locations throughout the Usa.[eight]
The U.S. Department of Health and Human being Services (HHS) projects the need for vii,987 primary care physicians in rural areas and shortages of dentists and psychiatrists besides.[9] Nationally, but 10 percent of physicians and eighteen percent of nurse practitioners (NPs) practise in rural locations, withal one-fourth of America's population resides in rural areas.[x] Rural populations are poorer and more likely to participate in regime aid, creating the potential for loftier need due to the Medicaid expansion in 26 states.[eleven] Geographical challenges affect the health of rural Americans through longer wait times, difficulty accessing intendance, long-distance travel, and limited resources.
The ACA reauthorized loan repayment and forgiveness, scholarships, increases in Medicare-funded Graduate Medical Education (GME) residency slots, funding for workforce planning, and increased funding for the Public Health Service. These are intended to reduce the rural shortages, but these programs accept historically achieved only limited success. Yet they have been the only initiatives to accost maldistribution.
The danger is that these shortages will result in increased morbidity and mortality for rural Americans. Solving the problem will likely require a epitome shift in educational admission practices, recruitment of more than personnel with rural experiences, payment reform in the public and individual sectors, and a much friendlier regulatory environment for medical do, including tort reform.
Disproportionate Ratios. Another personnel supply trouble is the disproportionate ratio of primary care physicians to specialists. Research suggests that the ideal ratio of specialists to master care physicians is 40 pct to fifty per centum in the healthiest nations.[12]A large gap in this ratio currently exists, with only one-third of physicians working in master care. In states with college ratios of specialists to principal intendance physicians, inquiry indicates increased costs and decreased quality of care.[13]
The ACA relies heavily on the concept of the Patient Centered Medical Home (PCMH) model and gratuitous preventive care. However, both models require enough primary care providers to evangelize services. This will be hard given the projected personnel shortages.[fourteen] The ACA's newly insured population is expected to require at least 8,000 additional master care physicians to come across their needs.[xv] Even with the utilize of nurse practitioners (NPs) and md assistants (PAs), projective shortages range from 20,400 to 45,000 master care physicians over the next decade.[16]
Prospective medical students exhibit less interest in chief intendance in part considering of a $three.v million income gap over a lifetime of work and the increasing debt of pupil loans.[17] Primary care physician payments would need to increase past $100,000 annually to meet the income levels of specialists.[eighteen] In both the public and the individual sectors, medical professionals are taking advantage of payment reforms. Medical education should include new incentives for master intendance. An emphasis on GME residency slots for primary care in the Medicare program might help to reverse the turn down.[19]
Higher Intensity of Care. "Patient vigil" is a measurement of the intensity of care required to treat a patient. The higher the acuity, the more care a patient requires. In terms of work flow, this means the number of medical professionals needed to care for a patient depends on the gravity or nature of the patient's medical status. Every bit the population ages, the number of patients suffering from chronic diseases volition increase significantly, requiring additional labor hours to ensure quality of care. Furthermore, chronic disease is affecting more Americans, not just the elderly. By 2025, nearly one-half of all Americans volition suffer from a chronic disease, resulting in a greater demand on the health care organisation.[xx]
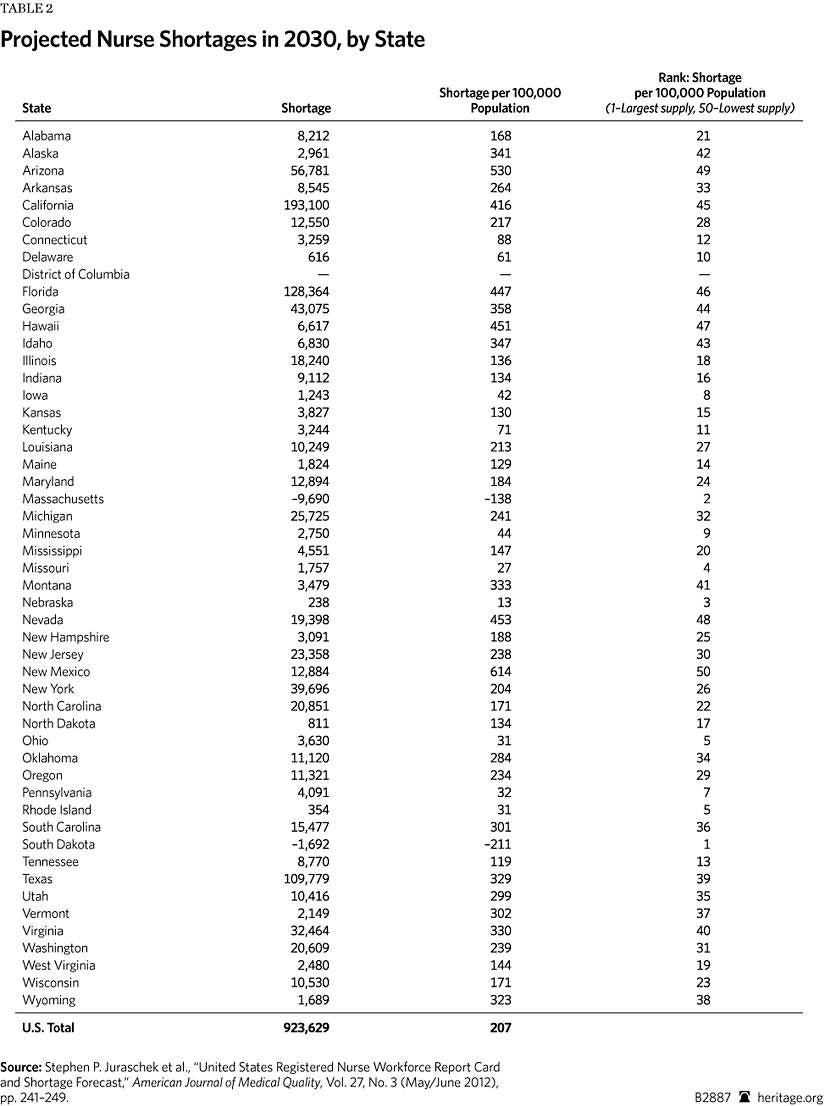
Looming Retirements. The aging population and crumbling workforce further complicate the ACA's implementation. Of the estimated 2.8 meg registered nurses (RNs) and the 985,375 physicians currently working, ane-third will likely retire in the adjacent decade.[21] Workforce projections anticipate a disquisitional shortage of between 91,500 to 130,000 physicians and the demand for an boosted 300,000 to i.2 million registered nurses by 2020.[22] The economical downturn of recent years has encouraged many professionals to stay in the workforce for financial reasons, but the additional stresses of the ACA will probable accelerate their exodus.
Younger physicians exhibit different attitudes toward their professional roles and responsibilities. A contempo workforce survey described physicians over the age of 50 as more defended and hardworking and their younger counterparts every bit disillusioned, less dedicated, and not every bit hardworking.[23] If this survey accurately reflects the younger workforce, medico productivity will probable decrease with increased retirements. There is little hope of coming together expected demand if productivity and efficiency do not increment.[24]
Telescopic-of-Practice Variability. In 2010, the Institute of Medicine (IOM) published a report recommending that all nurses practice to "the full extent of their instruction and training."[25] Advanced practice registered nurses (APRNs) are not just NPs educated in primary care, but trained professionals who provide services in multiple specialties. Many are certified as nurse anesthetists, nurse midwives, and clinical nurse specialists. While PAs are divers equally "part of a team" with supervising physicians, APRNS are trained to provide autonomous intendance for a focused population, such as principal intendance, pediatric, mental health, and critical care.[26]
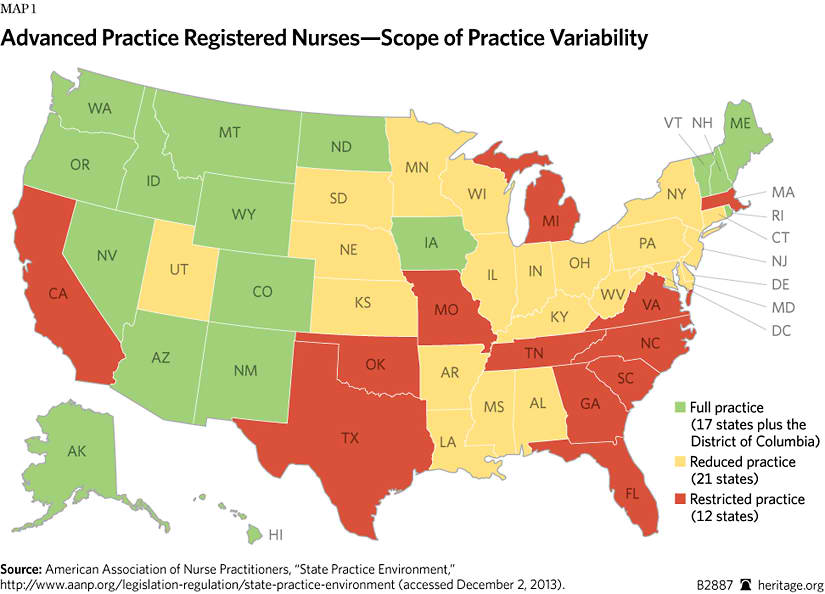
Currently, scope-of-practice laws vary widely from country to country. Seventeen states and the District of Columbia allow full practice by APRNs without oversight by physicians. Another 21 states qualify reduced practise by allowing APRNs to practice in collaboration with a physician, and 12 states restrict practice requiring collaboration, oversight, and supervision past a physician.[27] The workforce shortage result will require states to reexamine their scope-of-practice laws.
Educational Pipeline. Currently, medical pedagogy institutions are unable to graduate the number of workers needed to guarantee broad access to medical care. Even with recent enrollment increases, demand will still outweigh the supply by 2025.[28] The training pipeline is backlogged, and qualified applicants are not gaining entrance to professional person schools. Bereft numbers of instructors, limited clinical sites, and budgetary constraints contribute to the rejection of qualified applicants.[29]
Medical schools reportedly accustomed 25,321 of 45,266 applicants in 2012 and are attempting to increase enrollment xxx percent by 2017.[30] While medical schools are increasing enrollment, the number of Medicare-funded GME slots is insufficient to complete the training process.[31] In 2012, the number of graduates exceeded residency slots for the first time. This shortfall volition produce a snowball event moving forward, creating notwithstanding another barrier to output.[32]
The American Clan of Medical Colleges is supporting legislation to increase the number of Medicare-funded residency slots, but fifty-fifty if the President signs the legislation, the shortfall of residency slots will persist at to the lowest degree through 2017.[33] Even if medical schools tin graduate more students, the lack of residency slots prevents graduates from practicing medicine.
Nursing is experiencing like dynamics. More than than 79,000 qualified applicants were turned away from nursing programs in 2012.[34] Complicating matters, the average salary for positions in nursing education is significantly lower than what these experts tin earn outside academia, making it difficult to recruit and retain key academic personnel. A survey by the American Association of Colleges of Nursing identified 1,358 unfilled total-time faculty positions for the 2013–2014 academic year, and 414 schools reported full-fourth dimension vacancies.[35]
Aging kinesthesia also poses a threat to medical education. The average historic period of associate nursing professors is 52, and the average banana professor is 49, while the average historic period of medical schoolhouse faculty is between 50 and 59.[36] Retirements are on the horizon, and whatever additional losses of kinesthesia volition increase the excess in the educational pipeline.
ACA Aggravating Workforce Stress
Without a stiff and growing workforce operating under better working conditions, the quality of patient intendance volition not improve. Wellness professionals worry about the ACA's affect on their workforces, and many are considering culling careers and opportunities. The ACA increases stress on private workers, organizations, and systems. Role of the problem is the overwhelming complexity of implementing the massive police, requiring them to meet new legal requirements while fulfilling professional obligations and meeting professional person expectations for high performance in delivering patient care. Rather than ease these problems, the ACA aggravates them.
Heavier Workloads. With millions of people entering the ranks of the insured combined with the decline in the growth of the wellness care workforce, doctors, nurses, and other medical professionals should expect their workload to increase dramatically. Increased safety issues and greater stress on workers will inevitably increase work demands.[37] The ACA's financial incentives for and penalties against doctors and other medical professionals are to exist tied to quality and functioning metrics, but with the diminished workforce, maintaining the sufficient ratios to ensure quality care will exist difficult.
Increased medical errors from fatigue, poorer outcomes, and even patient death are a direct event of workforce stress and heavy workloads.[38] Historically, vulnerable populations with complex medical weather, such as the elderly and African Americans, are afflicted more than. Heavy workloads can even increase health care disparities.[39] With the newly insured under the ACA anticipated to increment the number of patients in the system with complex medical problems, meeting their needs will require a significant investment of human being capital. Otherwise, the additional strain will overwhelm already overstressed medical professionals.[twoscore]
More Paperwork. In addition to the sheer number of new patients in the system, the ACA intensifies the regulation of an already overregulated system. The enormous paperwork requirements will reduce time spent with patients and significantly increase the costs of providing care. Complying with requirements to report quality measures and patient outcome data will require hiring additional staff and investing in infrastructure to complete the necessary tasks to ensure the highest level of payments.[41] Afterwards the 2006 Massachusetts health reform, the employment of authoritative personnel in health care grew past more than than 18 percent—a rate six times college than the growth in employment of physicians and nurses.[42]
Since 1997, the federal government has issued 100 new or revised federal health intendance regulations, and this does non include countless country and local regulations. Medical professionals were already drowning in an ocean of paperwork. A 2001 written report for the American Hospital Association plant that hospital officials spent xxx minutes to one hr on paperwork for every hour spent on patient care in a Medicare-funded hospital.[43] For example, one 60 minutes of patient intendance in the emergency room required one hr of paperwork, and one hr of patient care in an acute care unit required 36 minutes of paperwork.[44]
The ACA has thus far added 109 distinct regulations. The time and effort to comply with these rules and regulations will equal an estimated 190 million hours of paperwork per year imposed on business and the wellness care manufacture.[45] Most of the estimated 13,000 pages of regulations are focused on health care institutions, and compliance with these rules will also reduce the time spent on direct patient intendance.[46] History suggests that this volition cause a significant loss of directly patient care hours—a worrisome problem in light of the projected shortages and an unacceptable and unnecessary burden on the workforce.
Health care paperwork and government regulations are already out of control. Health care professionals went into medicine to assistance people, not to fill out government forms. Every infinitesimal and dollar spent on paperwork is a minute and dollar taken abroad from patient care. By adding 190 million hours of paperwork per yr, the ACA volition worsen practise conditions and exacerbate the health care workforce shortage, increasing costs and robbing health care professionals of the time needed to intendance safely for patients.[47]
The Penalty Problem. The ACA relies heavily on mandates, penalties, and bonus reimbursements for compliance with its regulatory standards. Even with attempts to improve performance over the past few years, 2,225 hospitals were penalized in 2013 under the Hospital Readmissions Reduction Plan (HRRP), office of the ACA legislation. The penalties totaled more than than $227 meg, and facilities located in poor regions where a college proportion of depression-income patients are treated were hardest hitting.[48] With the HRRP and the reduction of Medicaid Disproportionate Share Hospital (DSH) payments, providers are experiencing significant cuts in revenue while trying to increase quality of care to meet or maintain the ACA'due south benchmarks. While physicians escaped a reduction in Medicare reimbursement rates in 2013, a 25 percent reduction is scheduled for 2014.[49] Nether current police, physicians are unlikely to avoid the payment rate reductions, endangering their fiscal margins.
With the new regulations, lower reimbursement rates, and required investments in technology, wellness care institutions and medical professionals will take difficulty breaking even. In fact, hospitals laid off 6,000 workers in 2012, and more than 3,000 workers were affected by buyouts, attrition, or reductions in hours.[fifty]
The new pay-for-operation standards will significantly touch hiring and retention of labor. If facilities cannot amend their quality scores, the reduced reimbursements will mean budget cuts, shutting down units and even closing hospitals. A recent study indicated that hospitals were more likely to incur penalties when nurse staffing levels were lower, merely the additional stress and strain combined with financial losses make reductions in workers likely.[51]
Increased Dissatisfaction and Burnout. Working in health care is difficult with adequate personnel, much less with the anticipated shortfall of workers. Increased work-related stress volition affect the mental and emotional health of medical professionals.
In a contempo survey, one-third of physicians would not choose medicine if given the selection to do it over once more, and almost 60 percent would not recommend medicine equally a career.[52] Physician well-existence is straight correlated with the ability to provide quality of care to patients. With doc dissatisfaction increasing the likelihood of doctors leaving the profession by ii to three times, Americans can await boosted labor losses.[53] The outlook is grim. A recent survey reported that 49 per centum of physicians intend to stop practicing medicine as soon as possible or plan to reduce the years that they piece of work in medicine.[54] Physician dissatisfaction, peculiarly burnout from overload and emotional stress, threatens reform efforts and patients' access to care.[55]
Workplace stress is also responsible for depression and burnout among nurses. Nurses working in overcrowded and understaffed units are more likely to experience depression and absenteeism, thus increasing the burden on other nurses.[56] Nurses identify emotional distress from patient care, workload, fatigue, burnout, and an unfriendly workplace equally reasons for leaving the profession.[57] The ACA does zero to relieve this trouble and may brand information technology worse.
Medical Professionals' Right of Conscience. Many health care professionals are concerned with profound moral and ethical issues that periodically arise in the health care field and worry near their traditional ability to practice their rights of conscience nether the ACA. This is not a new trouble.
The Obama Assistants all simply rescinded the Bush-league Administration'south initiatives to protect health care workers. Thus, in many concrete circumstances, workers with religious or moral objections to sure medical treatments or procedures are left without specific, explicit protections, and the Obama Assistants has thus far blocked legislation that attempts to correct the trouble.
Current law contains no enforcement provisions. Meanwhile, HHS has blatantly disregarded right of censor by mandating insurance funding of abortion-inducing drugs, contraception, and sterilization.[58] Right-of-censor supporters have focused on reproductive rights and the rights of the unborn child, but the ethical concerns are broader. For example, these concerns can cover annihilation that a medical professional or wellness worker finds to be a "major transgression" that is "well-defined" and "accepted by a cultural group."[59]
Polling supports medical professionals' ethical concerns. Correct of conscience is supported by 63 per centum of the American public, and 87 per centum agree that health care workers should non be forced to participate in procedures that go against their moral conscience. In a survey of organized religion-based providers, 39 percent confirmed discrimination for using right of conscience and 95 percent indicated that they would leave the medical profession before they are forced to violate their censor.[sixty]
ACA legislation creates a bulwark to Medicare's physician–patient human relationship through the Independent Payment Informational Board defining what treatments can or should exist funded and insurance companies and government program officials determining what treatments are allowable. Wellness care workers are voicing growing business over the implication of these barriers to ethical patient care. The marginalization of physicians and practitioners created by ACA legislation compromises safety and increasingly infringes on the ethical and moral obligations defined by the medical professions.
With the ACA-based contraceptive mandate and states considering measures to forcefulness health intendance workers to provide services regardless of moral objections, Americans take every reason to worry nearly efforts to violate the correct to religious liberty and the right of conscience.[61] The wellness professions require workers to adhere to a code of ethics and to maintain the highest moral and upstanding standards. Without explicit legal protections, health care workers volition be forced to choose between violating their personal moral and ethical beliefs or losing their jobs. Without legislative guarantees and enforcement provisions, wellness intendance workers face bigotry.
The Effects on Wellness Care Delivery
In response to increased regulatory burdens, health care stakeholders are changing concern practices. Ensuring viability in the new marketplace requires strategic planning and a vision of the time to come. A reevaluation of market place standing, labor costs, and current infrastructure is essential to ensuring solvency as the ACA is implemented.
Mega Wellness Intendance. Hospitals, individual physicians, group practices, and other health care businesses are merging and consolidating to remain strong in the marketplace. Mergers and acquisitions reduce overhead costs for billing and claims while spreading out the fiscal hazard and increasing market share. This gives them greater negotiating power with insurers, other hospitals, physicians, and government entities.[62] Horizontal and vertical consolidation in 2011 included 432 mergers involving 832 hospitals. At to the lowest degree 60 per centum of hospitals are now in a system.[63] In Massachusetts, for case, conglomerates testify lower costs of doing business merely increased costs for consumers and insurers—a troubling trend if it holds nationwide.[64]
While alliances help to increase quality and efficiency through coordination of care, some contend that consolidation and mergers can besides lead to monopolies in the marketplace. This raises anti-trust concerns. Consolidated systems may too lead to a reduction in quality as market consolidation eliminates the competitive incentives to ameliorate care.[65]
Physicians are selling practices, moving into larger physician groups, and seeking employment at hospitals. Frustrated with increased regulation, the financial costs of practice, liability, continually increasing workloads, and the overall stress of the workplace, physicians are choosing to forgo independent practise. By 2011, 50 percent of physicians were working for hospitals, insurers, or corporations—a significant change in the landscape of intendance delivery of a magnitude non seen since the 1990s.[66] The shift of physicians to hospital payrolls increases operating costs while decreasing the bottom line and increasing prices for consumers and payers.[67]
Directly-Care Models. Legitimate concerns about the workforce shortage, burdensome regulations, reduced fourth dimension with patients, and government involvement in the medico–patient relationship have prompted health care providers to begin changing contained practice models. Cash-only practices are popping upward effectually the country with many posting cost lists and requiring up-forepart payment for services. While the number of cash-merely practices is minor, do conversions have been rising for the past few years. Physicians who follow this route significantly reduce overhead costs past eliminating patient billing and claims, freeing them to set their ain prices and care for the patients in the manner that they encounter fit.[68] No insurance visitor or third party interferes with their decisions nigh treatments or care.
An estimated 1-third of physicians were anticipated to move to such a subscription-based practice model by the end of 2013. Direct pay and "concierge intendance" are subscription-based models in which patients pay a monthly or annual fee. Fees vary widely depending on services provided. Concierge practices provide a college level of service including care coordination and helping patients to negotiate the system while directly-pay practices provide more than limited services, such as aforementioned-mean solar day appointments and additional admission to doctors via phone or eastward-mail.[69] Patients pay a exercise or membership fee with a contract between the doctor and patient guaranteeing priority access and services added to basic care.
In most cases, patients are expected to retain insurance to comprehend fees for the physician'due south bones services. Many of the practices take individual insurance, Medicare, and Medicaid. The HHS has warned about such practices in the past, and as the market place for culling admission increases, there is concern that government will arbitrate to restrict or prohibit such practice models. Currently, as long as physicians can bear witness that the services existence paid for by the subscription fee are above and beyond the services that the md is contracted to provide through the private insurance or regime-run programs, they can avoid penalties for "double billing" or violations related to the insurance contracts.[70]
With subscription-based models, physicians can opt to limit or reduce the console of patients allowing for individualized, unhurried care with a guaranteed baseline income. In fact, some insurance companies are building plans for employers that allow individuals to purchase the concierge option for increased admission and payments.[71] While the cash-but, concierge care, and subscription-based models all attempt to safeguard the individual rights of the provider and patient while mitigating fiscal loss, the increasing number of these practices will touch affordability and accessibility for Americans. Innovative new practice models will guarantee access for those who can beget it.
Unintended Consequences. Adding up to 34 million patients to an insurance and commitment system that is already struggling with workforce shortages cannot avert adversely affecting patient admission and quality of intendance. The ACA cannot by itself guarantee access or increased quality of care through the mandated buy of all-inclusive insurance policies. In fact, the unintended consequences of the ACA's complexity will ripple throughout the health intendance sector.
Quality Health Care. Quality of care has been a major focus in health care in the U.S. for many years, and America's medical professionals have continually tried to ameliorate practice and provide the best care in the world. Nonetheless, the results accept been uneven.
The ACA approach to guaranteeing quality is to move the medical workforce from the fee-for-service model of health care reimbursement to pay-for-performance. Pay-for-performance is an umbrella term for initiatives that give incentives or penalties measured by patient outcomes and readmission rates.[72] The research shows that the number of physicians in a country is associated with better quality and improve outcomes.[73] Equally the workforce shortages worsen, the quality of intendance in states with fewer physicians overall will endure. States with higher physician-to-resident ratios will fare better nether the ACA's pay-for-functioning system, increasing inequality and disparity in the nation.[74]
While the concept of pay-for-performance shows some merit in reducing cost, transforming the system could prove difficult with the current penalties and reductions in reimbursement rates. Inadequate staffing levels significantly impact quality of care.[75] Low nurse staffing levels and college nurse-to-patient ratios have been shown to increase morbidity and mortality.[76] Working weather—such every bit increased pressure to perform, workforce shortages, and increased demand for services—will negatively affect health care institutions in the pay-for-performance arrangement.
A recent survey reported that "40 percent of hospitalists are already seeing heavy workloads that upshot in unsafe conditions, delays in patient admissions and discharge, and failure to talk over treatment options."[77] Hospitals and providers with more express resource and medical professionals working in economically depressed areas may take difficulty meeting benchmarks of progress if their payments are further reduced nether the ACA.[78] Strained finances, limited operating budgets, and staff layoffs—aggravated past ACA financial penalties and payment reductions—will cause a downward screw of low operation. The Role of the Actuary in the Centers for Medicare and Medicaid Services, among others, has already projected that more hospitals will be operating in the red or hovering on the brink of insolvency.
Admission to Health Care. Greater access to health intendance is a central ACA goal, but heavier demand for services volition probable create a bottleneck in access. Individuals on the exchanges will probable feel a narrowing of networks and express providers. In a survey by Jackson and Coker, 44 percent of physicians indicated that they volition not participate in the exchanges.[79] A survey by the Medical Group Management Association found that 64 percent of practices are concerned with the regulatory burdens, and 2 out of three practices indicated that reimbursement rates were lower than commercial rates, heightening concern about participation. The negative impact on practice decisions and fiscal instability is motivating many physicians to avoid contracting with health plans in the exchanges.[lxxx]
For example, a recent survey of 8,000 doctors in Massachusetts revealed a severe shortage that affected patient admission to care.[81] Even though Massachusetts has one of the highest doc-per-resident ratios in the nation, the land needs an increase of 2.8 percent in the employment level of doctors and nurses to secure the requirements of the reform.[82] In a country that was better equipped to absorb the impact than most in the nation, worker shortages go along to inhibit access to care. States with a low md-per-resident ratio (e.g., Nevada, Arkansas, Oklahoma, and Georgia) and states with more rural locations and limited access to the medical teaching pipeline will face critical shortfalls.[83]
Although many residents of urban areas may feel but a slight change, Americans living in more than rural locations will bear the brunt of the shortage. Long waits will become common. In fact, await times for new patients in some counties in Massachusetts take increased to 128 days for internists and 58 days for family do physicians, leading to greater apply of emergency rooms.[84] Half of primary intendance physicians are not accepting new patients, and the wait to see a gastroenterologist in Franklin County is 213 days.[85]
While many Americans will purchase insurance on heavily regulated exchanges, insurance itself does non guarantee access to or quality of care. Exchange plans with narrow networks invariably hateful express access to specialists and world-class treatment programs. Patients can lose choices in treatment and intendance.[86] Hospitals are closing, and rural hospitals and critical access facilities are increasingly at risk for closure. Many hospitals are requiring upward-front end payment of deductibles and co-pays for not-emergent services, further limiting admission and delaying care.[87]
A New Wellness Care Calendar
The ACA requires millions of Americans to enroll in health insurance, but the care delivery system is unprepared to absorb the influx of Americans seeking care. The ACA's new pressures will exacerbate attrition from burnout and dissatisfaction, worsening the existing shortage. Health care is a labor-intensive sector. The triple aim of increased quality and satisfaction, reduced costs, and increased health tin can be guaranteed only with an efficient workforce that is big plenty to accommodate the needs of a growing and aging population.[88] Solutions to the existing problems will require innovation in medical educational activity and preparation, improved delivery of care, and implementation of policies to retain the existing health intendance workforce.
Improve Teaching. Public policy is not the answer to all of the bug facing the medical professions. Many problems are endemic to professional person grooming, and the terms and conditions of grooming and educational activity should remain the responsibility of the professions.
Educational financing should reflect a amend balance between primary intendance and specialty practices, increasing graduates of all health professions and providing financial incentives for faculty. If medical and other health care students seek relief to reduce the financial burdens of their professional education, they should expect to serve persons in areas with serious shortages of medical personnel. A 2013 medical schoolhouse graduate accumulated an estimated $162,736 in debt past graduation. To make medical practice more attractive, policymakers demand to address some pressing issues, such as limiting tort liability and other constraints created by the debt load.[89]
Medical and professional colleges should prefer admissions criteria that attract students from rural areas, and the curriculum should address the challenges of practice in a rural environment. Admissions officers should identify students from rural areas and those planning to do in rural areas or master care. Wellness professionals should incorporate interprofessional education to increase efficiency and productivity, promote coordination of care, and hold training exercises in teamwork. Increasing worker productivity will require strategic planning and partnerships to increase output of highly competent providers of care while addressing the maldistribution and disproportionate ratio of wellness care workers.
Congress should likewise reevaluate the current Graduate Medical Education program. It is imperative to ensure available residency slots for the projected medical student enrollment. GME strategic planning should focus on rural and underserved communities and create additional slots for specialties with the highest projected shortages, such as primary care.
Congress should besides ameliorate Championship VIII Nursing Workforce Development. Programs funded through this initiative have contributed to an overall increase in the number of faculty and graduates of nursing schools.[90] Congress should evaluate the ACA'southward Graduate Nurse Education (GNE) pilot programme before providing additional funding. Time to come GNE programs should consider emphasizing rural didactics and primary care specialties to target specific distribution and shortage problems. Nursing educators need to streamline the curriculum to ensure that students are prepare for work when they graduate.
As with many other areas of public policy, Congress should refrain from bold responsibilities that are best left to state legislators, particularly where state nursing shortages are astute. In these cases, country legislators should prepare priorities and fund, as advisable, nursing schools in their states based on their citizens' needs.
Remove Barriers to Access. Telescopic-of-practice rules can contribute to the cost and inefficiency of the health care system, creating another barrier to patient admission to care.
In a national survey of physicians and nurse practitioners, a majority of respondents indicated that having more nurse practitioners would better timeliness of intendance and admission.[91] A written report deputed by Massachusetts encouraged greater use of NPs and PAs, estimating that reducing restrictions would relieve the state $four.ii billion to $eight.4 billion over 10 years.[92] While physicians are concerned with quality of care and, of form, a reduction in their market share, no evidence suggests that using APRNs negatively affects patients or physicians. Nursing, the largest segment of the wellness intendance workforce, should be "full partners" with other health professionals in the improvement of the health care arrangement.[93]
Dr. Darrel Due east. Kirch, Md, principal executive officer of the American Association of Medical Colleges, recently stated that the medical customs needs to railroad train an additional four,000 doctors per year "while besides embracing the roles in which other professionals can serve."[94] The impending shortage and the crumbling population demand a hard await at innovative models of intendance. The National Governors Association has come out in support of reexamining the scope-of-practice issues, and consumers are open to "a greater function for of md assistants and nurse practitioners" in the health care organisation.[95]
Entrenchment of professional organizations has undercut reform in many states, fifty-fifty though the looming shortages will necessitate the full employ of APRNs and other non-medico providers. Insurance companies and government agencies should remove obstacles to certification, eliminating payment bug. State legislators should examine the potential function of APRNs equally a way to increment access and achieve additional savings. Given the current critical juncture of need and supply of medical services, it is essential to ensure that all hands are on deck to care for the surge of patients.
Promote Efficient Care Commitment. Human capital is the backbone of the wellness care industry. Providing wellness care is labor intensive, and recruiting and retaining a sufficient workforce are essential. Strengthening the workforce supply should be coupled with innovation in role and chore allocation.[96] Efficiency and productivity volition aggrandize the workers' capacity to deliver loftier-quality patient intendance.
Achieving operational efficiencies among medical professionals will crave systematic analysis.[97] To increase care coordination and improve work flow, professionals should pursue team-based collaboration.[98] This means health professionals should define the necessary tasks of their own professions and be ready and able to delegate tasks outside of their profession to other personnel. Workforce shortages hogtie health care leaders to invent new ways to employ limited personnel efficiently to meet increased demands.
Improve the Practice Environment. Increasing retention will require greater incentives. Incentives should include a mix of public policies, such as reducing liability through tort reform, Medicare payment reform, and reduced federal revenue enhancement rates. In the private sector, health care businesses will need to apply the almost constructive methods of attracting, hiring, and retaining workers.[99] Retaining talent will require extensive human being resources planning and incentivizing through benefits, education and career advocacy, profit sharing, and workforce protections. Agile interventions to preclude work overloads and strategies for stress management will reduce attrition and costly replacements and ensure acceptable supply. Workers demand to exist protected physically, emotionally, and psychologically to ensure a healthy workforce.
Finally, wellness care workers should non be forced to cull between post-obit their moral conscience and obeying potentially immoral orders of their superiors. Congress tin can contribute to workforce well-being by enacting legislation that explicitly guarantees the right of censor and protects health care workers. Meanwhile, states should consider legislation that protects patients and workers from heavy workloads in state hospitals and other publicly funded institutions.
The Futurity of Health Care in the Residual
The viability of high-quality health care under the ACA is in doubt. The emerging health intendance workforce shortage, while rooted in trends that preceded the ACA, is non alleviated by the new health law. If these trends go on, they will go an insurmountable obstacle to the ACA'due south success and damage the quality of intendance for millions of Americans. In short, Americans need more than doctors, nurses, and other medical professionals.
Major provisions of the ACA were implemented in January 2014. With the rocky showtime to the exchange enrollment, the reduction in health plan competition in the exchanges, the emergence of narrow networks of doctors and other medical providers, and the rate shock of higher premiums and deductibles, more Americans oppose the new health law than support it. If these initial issues plough into cascading failures accompanied past massive disruptions of existing coverage and intendance, Congress will be forced to act.
Health care policy is no longer abstract when it directly affects the personal lives and health of millions of Americans. Under the ACA, Congress has prescribed a detailed federal office over health care financing, but financing directly and immediately affects the delivery of health care and how Americans access that care. Thus far, the ACA has delivered higher health insurance premiums, higher deductibles, and less competitive health insurance markets. This does not bode well for care delivery, particularly if it means increased waits, rationing of intendance, limited or no access, and poor quality of care. Americans' individual lives and their health decisions should be spared the consequences of such incompetent intrusions.
Sensible changes in health intendance policy could fix the problems of the few without harming the care of the many. Wellness care reform legislation should follow the principle primum non nocere ("start do no impairment") by carefully targeting the root of the problem, not by granting vast regulatory power to unaccountable government officials who consequence arbitrary edicts.[100] Every mean solar day the ACA is the "law of the state" risks permanent damage to the wellness care sector of the economy and the lives of Americans.
There is no shortage of policy prescriptions for rational and profoundly consequential health care reform: portability of insurance, cost transparency, taxation reform, tort reform, deregulation, payment reform, and the elimination of artificial barriers to coverage and intendance. Meanwhile, the ACA's unintended consequences cannot be ignored any longer. Americans should have the right of self-determination in health care. As the first step to secure that right, Congress must repeal this toxic law.
—Amy Anderson, DNP, RN, CNE, is a Graduate Wellness Policy Beau in the Center for Health Policy Studies at The Heritage Foundation and an Assistant Professor of Nursing at the Academy of Arkansas at Trivial Rock.
[one] Joe Cantlupe, "'Alarming' Physician Shortages Prevarication Alee," HealthLeaders Media, November 14, 2013, http://world wide web.healthleadersmedia.com/impress/PHY-298361/Alarming-Physician-Shortages-Prevarication-Ahead (accessed November 18, 2013).
[2] Stephen M. Petterson et al., "Projecting The states Primary Care Physician Workforce Needs: 2010–2025," Register of Family Medicine, Vol. ten, No. 6 (November/Dec 2012), pp. 503–509, and Kathleen Sebelius, "ACA Gets Care to Those in Most Need," Albuquerque Periodical, September 19, 2012, http://www.hhs.gov/secretary/almost/opeds/aca_care_to_those.html (accessed Oct vii, 2013).
[iii] Association of American Medical Colleges, Centre for Workforce Studies, "Contempo Studies and Reports on Doc Shortages in the United states of america," Oct 2012, https://www.aamc.org/download/100598/data/ (accessed January 28, 2014).
[iv] Robert Schlesinger, "U.Due south. Population 2013: More than Than 315 One thousand thousand People," U.S. News and World Report, December 28, 2012, http://www.usnews.com/stance/blogs/robert-schlesinger/2012/12/28/united states of america-population-2013-more-than-315-1000000-people (accessed October 15, 2013).
[5] Federal Interagency Forum on Aging-Related Statistics, "Population," http://world wide web.agingstats.gov/Main_Site/Data/2012_Documents/Population.aspx (accessed November 19, 2013).
[half-dozen] Noesis@Wharton, "Can the U.S. Meet Its Crumbling Population's Wellness Care Needs?" University of Pennsylvania, March 18, 2013, http://knowledge.wharton.upenn.edu/article/can-the-u-s-come across-its-aging-populations-health-care-needs/ (accessed Oct 11, 2013).
[7] Petterson et al., "Projecting United states Master Care Doctor Workforce Needs: 2010–2025."
[viii] Mark P. Doescher et al., "Persistent Master Health Care Shortages Areas (HPSAs) and Health Care Access in Rural America," Rural Health Research Center, September 2009, http://depts.washington.edu/uwrhrc/uploads/Persistent_HPSAs_PB.pdf (accessed Oct 17, 2013).
[9] Council of State Governments, "Health Care Workforce Shortages Critical in Rural America," May iv, 2011, http://knowledgecenter.csg.org/kc/content/health-care-workforce-shortages-disquisitional-rural-america (accessed October 11, 2013).
[ten] Ibid. and National Rural Health Clan, "What'south Dissimilar About Rural Wellness Intendance," http://world wide web.ruralhealthweb.org/become/left/about-rural-wellness (accessed November xix, 2013).
[11] Council of Land Governments, "Health Care Workforce Shortages Critical in Rural America."
[12] Jerry Kruse, "Saving Medicare: 'It's the Workforce Stupid!'" Register of Family Medicine, Vol. 4, No. 3 (May 1, 2006), pp. 274–275.
[13] Frank Diamond, "Specialists Putting Mark on Strained Primary," Managed Intendance, July 2010, http://www.managedcaremag.com/archives/1007/1007.primarycare.html (accessed October xviii, 2013).
[xiv] Kruse, "Saving Medicare."
[xv] Elayne J. Heisler, "Physician Supply and the Affordable Care Deed," Congressional Research Service Report for Congress, Jan 15, 2013, http://op.bna.com/hl.nsf/id/myon-93zpre/$File/crsdoctor.pdf (accessed January 23, 2014).
[16] U.South. Department of Health and Human Services, Agency for Healthcare Research and Quality, "The Number of Nurse Practitioners and Physician Assistants Practicing Chief Intendance in the U.s.a.," Oct 2011, http://www.ahrq.gov/inquiry/findings/factsheets/primary/pcwork2/index.html (accessed October four, 2013); Emily R. Carrier, Tracy Yee, and Lucy B. Stark, "Matching Supply to Demand: Addressing the U.Due south. Primary Care Workforce Shortage," National Found for Wellness Intendance Reform Policy Analysis No. 7, Dec 2011, http://world wide web.nihcr.org/PCP_Workforce (accessed January 27, 2014); and U.S. Department of Wellness and Human Services, National Center for Health Workforce Analysis, "Projecting the Supply and Demand for Primary Care Practitioners Through 2020," Nov 2013, http://bhpr.hrsa.gov/healthworkforce/supplydemand/usworkforce/primarycare/projectingprimarycare.pdf (accessed February 5, 2014).
[17] Bryan T. Vaughn et al., "Can We Close the Income and Wealth Gap Between Specialists and Chief Care Physicians?" Wellness Affairs, Vol. 29, No. five (May 2010), pp. 933–940, and Robert L. Phillips Jr. and Barbara J. Turner, "The Side by side Stage of Championship Seven Funding for Training Chief Care Physicians for America's Health Care Needs," Annals of Family Medicine, Vol. 10, No. 2 (March/Apr 2012), pp. 163–168, http://world wide web.annfammed.org/content/10/2/163.full (accessed November 19, 2013).
[xviii] Vaughn et al., "Can We Close the Income and Wealth Gap?"
[19] Phillips and Turner, "The Next Stage of Championship VII Funding."
[20] Partnership to Fight Chronic Disease, "The Growing Crunch of Chronic Illness in the United states," http://www.fightchronicdisease.org/sites/fightchronicdisease.org/files/docs/GrowingCrisisofChronicDiseaseintheUSfactsheet_81009.pdf (accessed October 28, 2013).
[21] Ibid. and Heisler, "Physician Supply and the Affordable Care Act."
[22] American Medical Association, "Adequate Funding of Graduate Medical Education (GME) Critical to Ensure Access to Current and Future Medical Services," 2013, http://world wide web.ama-assn.org/resources/doc/washington/graduate-medical-educational activity-action-kit.pdf (accessed October 25, 2013); Atul Grover and Lidia M. Niecko-Najjum, "Building a Health Care Workforce for the Futurity: More Physicians, Professional Reforms, and Technological Advances," Health Affairs, Vol. 32, No. eleven (November 2013), pp. 1922–1927; Stephen P. Juraschek et al., "United States Registered Nurse Workforce Written report Carte du jour and Shortage Forecast," American Periodical of Medical Quality, Vol. 27, No. 3 (May/June 2012), pp. 241–249; and American Association of Colleges of Nursing, "Sequestration: Estimating the Impact on America's Nursing Workforce and Wellness Care Discoveries," http://www.aacn.nche.edu/regime-affairs/AACN-Sequestration-Factsheet.pdf (accessed January 28, 2014).
[23] Health Cardinal, "Doctors Leaving Practice."
[24] Knowledge@Wharton, "Can the U.S. Run into Its Crumbling Population'south Health Care Needs?" and David I. Auerbach et al., "The Nursing Workforce in an Era of Health Care Reform," New England Journal of Medicine, Vol. 386, No. sixteen (April 18, 2013), pp. 1470–1472, http://www.nejm.org/doi/full/10.1056/NEJMp1301694 (accessed January 28, 2014).
[25] National Academies, Institute of Medicine, "Time to come of Nursing: Leading Change, Advancing Health," 2010, http://www.iom.edu/~/media/Files/Report%20Files/2010/The-Hereafter-of-Nursing/Future%20of%20Nursing%202010%20Recommendations.pdf (accessed October 15, 2013).
[26] Marty Stempniak, "Endmost the Primary Intendance Gap," H&HN, March 2013, http://www.hhnmag.com/mag/2013/March2013.dhtml (accessed January 28, 2014).
[27] American Association of Nurse Practitioners, "2013 Nurse Practitioner State Practise Environment," 2013, http://www.aanp.org/images/documents/country-leg-reg/stateregulatorymap.pdf (accessed Nov 12, 2013).
[28] Association of American Medical Colleges, "Contempo Studies and Reports on Physician Shortages in the United states."
[29] American Association of Colleges of Nursing, "New AACN Information Prove an Enrollment Surge in Baccalaureate and Graduate Programs among Calls for More Highly Educated Nurses," http://www.aacn.nche.edu/news/manufactures/2012/enrollment-data (accessed October 18, 2013).
[30] Association of American Medical Colleges, "Medical Schoolhouse Enrollment on Pace to Reach 30 Percent Increase past 2017," May 2, 2013, https://world wide web.aamc.org/newsroom/newsreleases/335244/050213.html (accessed November 17, 2013), and "2012 Applicant and Enrollment Data Charts," November 2, 2012, https://www.aamc.org/download/310122/data/2012applicantandenrollmentdatacharts.pdf (accessed Oct xviii, 2013).
[31] Association of American Medical Colleges, Heart for Workforce Studies, "Results of the 2012 Medical School Enrollment Survey," May 2013, https://members.aamc.org/eweb/upload/12-237%20EnrollmSurvey2013.pdf (accessed October 18, 2013).
[32] Ibid.
[33] H.R. 1201 would add an additional 15,000 Medicare-funded residency slots by 2019. Clan of American Medical Colleges, "Grooming Tomorrow'south Doctors Today Act (H.R. 1201)," November 14, 2013, https://www.aamc.org/download/355920/data/trainingtomorrowsdoctorstodayact.pdf (accessed February v, 2014).
[34] Policy Brief, "Sidelining Healthcare Quality: Capacity Barriers in America's Nursing Schools," American Association of Colleges of Nursing, Oct 22, 2013, https://www.aacn.nche.edu/regime-affairs/Capacity-Barriers-FS.pdf (accessed Feb 10, 2014).
[35] Ibid. and Di Fan and Yan Li, "Special Survey on Vacant Faculty Positions for Academic Yr 2013–2014," American Association of Colleges of Nursing, http://www.aacn.nche.edu/leading-initiatives/research-information/vacancy12.pdf (accessed October 18, 2013).
[36] American Association of Colleges of Nursing, "Strategies to Reverse the New Nursing Shortage," http://www.aacn.nche.edu/publications/position/tri-council-shortage (accessed October 18, 2013).
[37] Henry J. Michtalik et al., "Touch on of Attending Dr. Workload on Patient Intendance: A Survey of Hospitalists," JAMA Internal Medicine, Vol. 173, No. 5 (March 11, 2013), pp. 375–377.
[38] Ibid. and Linda H. Aiken et al., "Infirmary Nurse Staffing and Patient Mortality, Nurse Burnout and Chore Dissatisfaction," JAMA, Vol. 288, No. 16 (October 23/30, 2002), pp. 1987–1993, http://www.nursing.upenn.edu/media/Californialegislation/Documents/Linda%20Aiken%20in%20the%20News%20PDFs/jama.pdf (accessed November twenty, 2013).
[39] J. Margo Brooks Carthon, "College Nurse Workloads Lead to Poorer Outcomes for Black Patients," Reflections of Nursing Leadership, October 26, 2012, http://www.reflectionsonnursingleadership.org/Pages/Vol38_4_RNews_Carthon.aspx (accessed October 23, 2013).
[twoscore] Karen Brown, "Mass. Health Intendance Reform Reveals Doctor Shortage," NPR, http://www.wbur.org/npr/97620520/mass-health-care-reform-reveals-dr.-shortage (accessed November 30, 2008).
[41] Liselotte N. Dyrbye and Tait D. Shanafelt, "Dr. Burnout a Potential Threat to Successful Wellness Care Reform," JAMA, Vol. 305, No. 19 (May 18, 2011), pp. 2009–2010.
[42] Douglas O. Staiger, David I. Auerbach, and Peter I. Buerhaus, "Health Care Reform and the Health Care Workforce—The Massachusetts Feel," The New England Journal of Medicine, Vol. 365, No. 12 (September 7, 2011), http://world wide web.nejm.org/doi/full/10.1056/NEJMp1106616 (accessed January 28, 2014).
[43] American Hospital Association, "Patients or Paperwork? The Regulatory Burden Facing America's Hospitals," http://www.aha.org/content/00-10/FinalPaperworkReport.pdf (accessed October 17, 2013).
[44] Ibid.
[45] U.S. Business firm of Representatives, Committee on Ways and Means, Committee on Instruction and the Workforce, and Commission on Energy and Commerce, "Obamacare Burden Tracker," http://waysandmeans.house.gov/uploadedfiles/aca_burden_tracker_final_5_6_13.pdf (accessed Oct 21, 2013), and Penny Star, "Obamacare Regulations Are 8 Times Longer Than the Bible," CNSNews.com, September 10, 2013, http://cnsnews.com/news/commodity/penny-starr/obamacare-regulations-are-8-times-longer-bible (accessed November xx, 2013).
[46] Grace-Marie Turner, "The New HHS Regulation Purge," National Review Online, February 5, 2013, http://www.nationalreview.com/corner/339869/new-hhs-regulation-purge-grace-marie-turner (accessed Oct 17, 2013).
[47] U.S. House of Representatives, "Obamacare Burden Tracker."
[48] The Advisory Lath Company, "CMS, The ii,225 Hospitals That Volition Pay Readmission Penalties This Yr," The Daily Conference, Baronial 5, 2013, http://www.advisory.com/Daily-Briefing/2013/08/05/CMS-2225-hospitals-will-pay-readmissions-penalties-next-year (accessed Oct 22, 2013).
[49] Alyene Senger, "Obamacare'south Impact on Doctors—An Update," Heritage Foundation Effect Brief No. 4024, August 25, 2013, http://world wide web.heritage.org/enquiry/reports/2013/08/obamacares-touch-on-doctors-an-update (accessed Nov 20, 2013).
[50] Jed Graham, "Infirmary Layoffs Selection Up as Obamacare Era Starts," Investor's Business Daily, July 19, 2013, http://news.investors.com/071913-664373-hospitals-cut-jobs-on-obamacare-medicare-medicaid.htm (accessed October 22, 2013).
[51] Norra MacReady, "College Nurse Staffing Levels May Mean Fewer CMS Penalties," Oct 10, 2013, http://www.medscape.com/viewarticle/812459 (accessed October 22, 2013).
[52] The Physicians Foundation, "A Survey of America's Physicians: Practice Patterns and Perspectives," http://www.physiciansfoundation.org/uploads/default/Physicians_Foundation_2012_Biennial_Survey.pdf (accessed October xi, 2013).
[53] Bruce E. Landon et al., "Leaving Medicine: The Consequences of Md Dissatisfaction," Medical Care, Vol. 44, No. 3 (March 2006), pp. 232–242.
[54] Jackson & Coker, "Survey: Physicians on the Affordable Intendance Act," November 2013, http://www.jacksoncoker.com/cmscontent/Emails/Surveys/ACA/images/Physician-Survey-Obamacare.pdf (accessed Nov 21, 2013).
[55] Dyrbye and Shanafelt, "Physician Burnout a Potential Threat to Successful Health Intendance Reform."
[56] Jennifer Larson, "The Human relationship Between Workplace Stress and Depression in Nurses," NurseZone, June 17, 2010, http://www.nursezone.com/Nursing-News-Events/more than-features/The-Human relationship-Between-Workplace-Stress-and-Depression-in-Nurses_34420.aspx (accessed October 28, 2013), and Brinda McKinney, "Withstanding the Force per unit area of the Profession," Journal for Nurses in Staff Development, Vol. 27, No. 2 (March/Apr 2011), pp. 69–73.
[57] Carol Isaak MacKusick and Ptlene Minick, "Why Are Nurses Leaving? Initial Findings from a Qualitative Study on Nursing Attrition," MedSurg Nursing, Vol. 19, No. vi (November/Dec 2010), pp. 335–340, http://world wide web.amsn.org/sites/default/files/documents/practise-resources/good for you-work-environment/resources/MSNJ_MacKusick_19_06.pdf (accessed January 28, 2014).
[58] Chuck Donovan, "Censor Regulations: HHS Stops (Just) Brusk of Rescission," The Heritage Foundation, The Foundry, February 18, 2011, http://blog.heritage.org/2011/02/18/conscience-regulations-hhs-stops-just-short-of-rescission/ (accessed November xx, 2013).
[59] Azgad Gilt, "Physicians' 'Right of Conscience'—Beyond Politics," Journal of Police, Medicine and Ideals, Vol. 38, No. i (Leap 2010), pp. 1073–1105.
[sixty] Freedom2Care, "Ii National Polls Reveal Broad Back up for Censor Rights in Health Intendance," Christian Medical Clan, http://www.cmda.org/WCM/source/Pollingsummaryhandout.pdf (accessed October 23, 2013).
[61] Denise M. Burke and Anna Franzonello, "Health Care Rights of Censor: A Survey of Federal and State Law," 2012, in Americans United for Life, Defending Life (Washington, DC: Americans United for Life, 2012), pp. 547–553, http://world wide web.aul.org/wp-content/uploads/2012/04/survey-fed-land-law.pdf (accessed October 23, 2013).
[62] Steven Syre, "two Big Physician Groups May Merge," The Boston Globe, April 22, 2011, http://www.boston.com/business/healthcare/articles/2011/04/22/two_of_massachusetts_largest_doctors_groups_in_merger_talks/ (accessed October 4, 2013).
[63] David Yard. Cutler and Fiona Scott Morton, "Hospitals, Market place Share, and Consolidation," JAMA, Vol. 310, No. eighteen (November 13, 2013), pp. 1964–1970.
[64] Robert Weisman, "Hospital Mergers May Drive Upward Toll," The Boston Globe, October 3, 2013, http://world wide web.bostonglobe.com/business/2013/10/02/health-care-leaders-warn-that-infirmary-consolidation-could-bulldoze-costs/ZAg3Wy0tomHOPK3UNiHw0J/story.html (accessed Oct 23, 2013).
[65] Tamara Hayford, "The Affect of Hospital Mergers on Treatment Intensity and Health Outcomes," Wellness Services Enquiry, Vol. 47, No. three (June 1, 2012), pp. 1008–1029.
[66] Jeffrey A. Vocalizer, "Denigrating Medicine: Obamacare Turns Physicians into Assembly Line Workers," Pittsburgh Tribune-Review, May xix, 2013, http://triblive.com/stance/featuredcommentary/3970198-74/medicare-private-doctors (accessed October 22, 2013).
[67] Weisman, "Hospital Mergers May Drive Up Cost."
[68] Bruce Kennedy, "More Doctors Are Switching to Cash-Only Practices," MSN Coin, June 13, 2013, http://money.msn.com/now/weblog--more-doctors-are-switching-to-greenbacks-only-practices (accessed Oct 22, 2013).
[69] Accenture, "Clinical Transformation: New Business Models for a New Era in Healthcare," September 27, 2012, http://www.accenture.com/us-en/Pages/insight-new-business-models-new-era-healthcare.aspx (accessed October 22, 2013).
[lxx] U.S. Authorities Accountability Office, Medico Services: Concierge Intendance Characteristics and Considerations for Medicare, August 2005, http://www.gao.gov/new.items/d05929.pdf (accessed November 21, 2013).
[71] Jen Wieczner, "Pros and Cons of Concierge Medicine," The Wall Street Journal, November 10, 2013, http://online.wsj.com/news/articles/SB10001424052702303471004579165470633112630 (accessed November 18, 2013).
[72] Julia James, "Health Policy Cursory Pay for Performance," Health Affairs, Health Policy Cursory, October 11, 2012, http://healthaffairs.org/healthpolicybriefs/brief_pdfs/healthpolicybrief_78.pdf (accessed November 21, 2013).
[73] Richard A. Cooper, "States with More Physicians Have Better-Quality Health Care," Wellness Affairs, Vol. 28, No. 1 (December 4, 2008), pp. 91–102.
[74] Ibid.
[75] Jack Needleman et al., "Nurse-Staffing Levels and the Quality of Care in Hospitals," New England Journal of Medicine, Vol. 346, No. 22 (May 30, 2002), pp. 1715–1722.
[76] Robert Fifty. Kane et al., "Nurse Staffing and Quality of Patient Intendance," U.South. Department of Wellness and Human Services, Bureau for Healthcare Enquiry and Quality Show Report/Technology Cess No. 151, March 2007, pp. 1–115, and ibid.
[77] Henry J. Michtalik, "The Impact of Hospitalist Workload on Patient Care," Medico's Weekly, August 22, 2013, http://www.physiciansweekly.com/hospitalist-workload-patient-intendance/ (accessed October 21, 2013).
[78] RAND Corporation, "Pay-For-Functioning Programs May Worsen Medical Disparities, Study Finds," ScienceDaily, May 10, 2010, http://www.sciencedaily.com/releases/2010/05/100504074843.htm (accessed November 21, 2013).
[79] Jackson & Coker, "Survey: Physicians on the Affordable Intendance Act."
[fourscore] Chris Jacobs, "Survey: Doctors May Non Participate in Obamacare Exchanges," The Heritage Foundation, The Foundry, October 10, 2013, http://blog.heritage.org/2013/x/x/survey-doctors-may-non-participate-in-obamacare-exchange-plans/ (accessed October eleven, 2013).
[81] Bob Salsburg, "Survey: Disquisitional Shortage of Primary-Intendance Doctors in Mass.," Lowell Lord's day, September 18, 2013, http://www.lowellsun.com/local/ci_24118927/survey-critical-shortage-primary-intendance-doctors-mass (accessed October 9, 2013).
[82] Staiger et al., "Health Care Reform and the Wellness Care Workforce."
[83] Salsburg, "Survey: Disquisitional Shortage of Master-Intendance Doctors in Mass.," and U.S. Department of Health and Human Services, National Heart for Health Workforce Analysis, The U.S. Wellness Workforce Chartbook, Nov 2013, http://bhpr.hrsa.gov/healthworkforce/supplydemand/usworkforce/chartbook/chartbookpart1.pdf (accessed Feb 10, 2014).
[84] Jim Kinney, "Massachusetts Medical Order: Waiting Times for Doctors Is Also Long," The Republican, July xv, 2013, http://www.masslive.com/business organisation-news/alphabetize.ssf/2013/07/massachusetts_medical_society_wait_times.html (accessed Oct 28, 2013), and Massachusetts Medical Club, "2013 MMS Patient Access to Care Report," July 15, 2013, http://www.massmed.org/patientaccess/ (accessed Oct 28, 2013).
[85] Massachusetts Medical Society, "2013 MMS Patient Access to Care Written report."
[86] Watchdog.org, "Top Hospitals Opt Out of Obamacare," U.South. News and World Study, October 30, 2013, http://health.usnews.com/health-news/hospital-of-tomorrow/articles/2013/10/thirty/top-hospitals-opt-out-of-obamacare (accessed November 22, 2013).
[87] Bob Herman, "Rural Healthcare Amidst Reform: Are Critical Access Hospitals Endangered?" Becker'south Hospital Review, September 25, 2013, http://www.beckershospitalreview.com/hospital-management-administration/rural-healthcare-amidst-reform-are-disquisitional-admission-hospitals-endangered.html (accessed November 21, 2013).
[88] Constitute for Healthcare Improvement, "The IHI Triple Aim," http://www.ihi.org/offerings/Initiatives/TripleAim/Pages/default.aspx (accessed November 12, 2013).
[89] Association of American Medical Colleges, "Medical School Education: Debt, Costs, and Loan Repayment Fact Card," October 2013, https://www.aamc.org/download/152968/information/debtfactcard.pdf (accessed November 22, 2013).
[90] American Association of Colleges of Nursing, "Testimony of the American Clan of Colleges of Nursing Regarding Fiscal Year 2013 Appropriations for the Title Viii Nursing Workforce Development Programs, the National Constitute of Nursing Research, and Nurse-Managed Health Clinics," testimony earlier the Subcommittee on Labor, Health and Human Services, and Educational activity, and Related Agencies, Committee on Appropriations, U.Due south. Firm of Representatives, March 29, 2012, http://www.aacn.nche.edu/authorities-affairs/cribbing-advancement/FY13House-LHHS-Testimony.pdf (accessed November 22, 2013).
[91] Karen Donelan et al., "Perspectives of Physicians and Nurse Practitioners on Primary Intendance Do, The New England Journal of Medicine, Vol. 368, No. 20 (May 16, 2013), pp. 1898–1906, http://dhhs.ne.gov/publichealth/Licensure/Documents/PerspectivesOnPrimCarePractice.pdf (accessed November 22, 2013).
[92] Christine Eibner et al., Controlling Wellness Intendance Spending in Massachusetts: An Analysis of Options, Rand Corporation, Baronial 2009, http://www.rand.org/content/dam/rand/pubs/technical_reports/2009/RAND_TR733.pdf (accessed October xv, 2013).
[93] National Academies, "Futurity of Nursing."
[94] Association of American Medical Colleges, "Report Shows Patients Would Consider a Greater Function for Medico Administration and Nurse Practitioners for Timely Access to Care," June 3, 2013, https://www.aamc.org/newsroom/newsreleases/343992/060313.html (accessed Oct 16, 2013).
[95] John 1000. Iglehart, "Expanding the Part of Avant-garde Nurse Practitioners-Risks and Rewards," The New England Periodical of Medicine, Vol. 368, No. xx (May 16, 2013), pp. 1935–1939, and Michael J. Dill et al., "Survey Shows Consumers Open to a Greater Role by Physicians Administration and Nurse Practitioners," Health Affairs, Vol. 32, No. 6 (June 2013), pp. 1135–1142.
[96] American Hospital Clan, "Workforce 2015: Strategy Trumps Shortage," January 2010, http://www.aha.org/content/00-10/workforce2015report.pdf (accessed October 28, 2013).
[97] Plant for Healthcare Improvement, "Gap Analysis: Where Exercise We Stand?" http://world wide web.ihi.org/offerings/Initiatives/Improvemaphospitals/Documents/IHIGapAnalysis.pdf (accessed Oct 28, 2013).
[98] National Health Service, Institute for Innovation and Improvement, "Role Redesign," 2008, http://world wide web.institute.nhs.great britain/quality_and_service_improvement_tools/quality_and_service_improvement_tools/role_redesign.html (accessed October 28, 2013).
[99] American Social club of Healthcare Human Resource Administration, "Alluring, Onboarding and Retaining Employees Within the Wellness Care Industry," e-News Brief, January 12, 2011, http://world wide web.naylornetwork.com/ahh-nwl/articles/index-v2.asp?aid=134767&issueID=22500 (accessed November 17, 2013).
[100] MedicineNet.com, MedTerms, s.five. "Primum non nocere," http://www.medterms.com/script/main/art.asp?articlekey=6110 (accessed November 22, 2013).

Source: https://www.heritage.org/health-care-reform/report/the-impact-the-affordable-care-act-the-health-care-workforce
Posted by: thompsonthencerest70.blogspot.com
0 Response to "What Is The False Claims Act And How Does It Impact Providers Of Health Care Services?"
Post a Comment